︎︎︎ previous next ︎︎︎
Building trust between dementia patients and their caregivers
Feb. - Apr. 2020
Dementia is a disease that requires constant and unpredictable adaptation that consumes everyone involved: patients, family, and caregivers. A few years after diagnosis, once the symptoms have become a daily obstacle, the demand on the family to care for the patient becomes too great and often a professional caregiver is hired. Along with the shifting challenges inherent with dementia, this caregiver must now build the trust necessary to provide proper care. I partnered with IBM to help overcome these challenges in caregiving using the affordances of machine learning.
TEAM
Eryn Pierce
Gloria Jing
Eryn Pierce
Gloria Jing
IBM WATSON HEALTH TEAM
Debi Ndindjock
Aisha Walcott-Bryant
Debi Ndindjock
Aisha Walcott-Bryant
OBJECTIVE
How might machine learning be used to
effectively assist a caregiver in maintaining
the autonomy of a patient through the stages
of dementia and increasing caregiver custody?
How might machine learning be used to
effectively assist a caregiver in maintaining
the autonomy of a patient through the stages
of dementia and increasing caregiver custody?
CONTEXT
Dementia is a chronic condition whose symptoms can vary drastically throughout its progression. This inconsistency makes it difficult to give medical care to patients and impractical to design any sort of hard and fast interventions. This burden often falls on a typically overlooked stakeholder: the caregiver, whether in the family or professional.
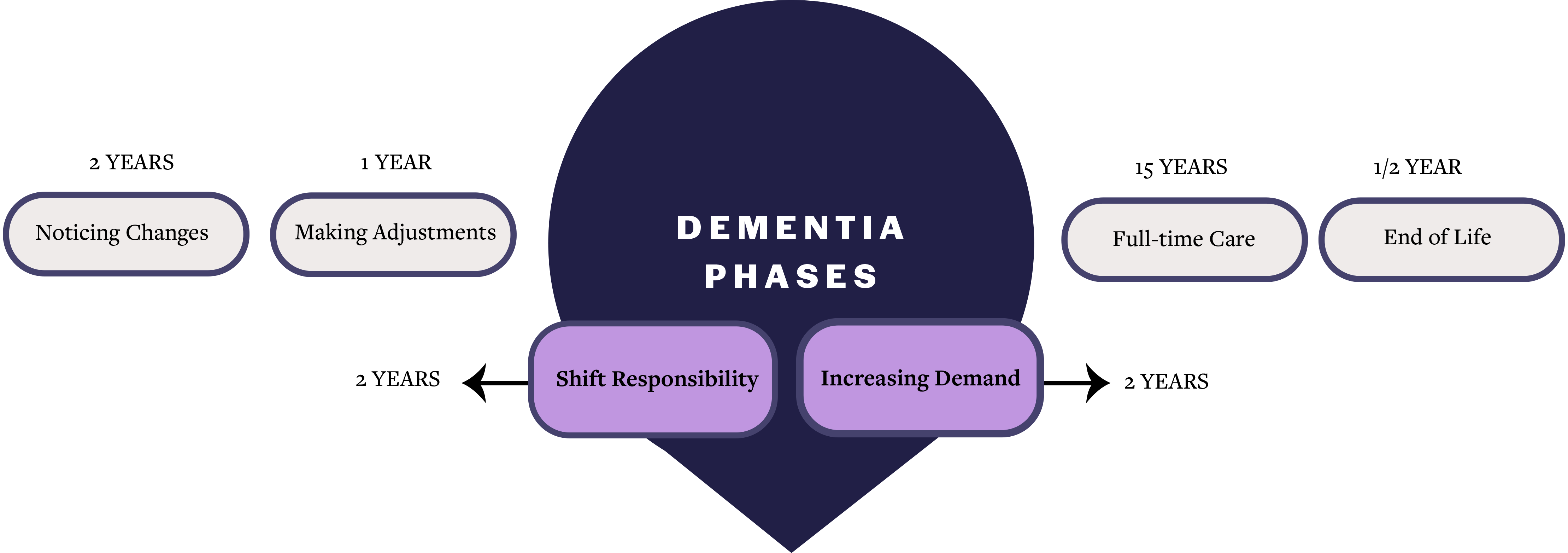
Needing to narrow down somewhere in the disease's timeline, My team and I decided to target the two intermediate stages of dementia caregiving (shifting responsibility and increasing demand) for multiple reasons. These stages mark the time between when symptoms are becoming a daily challenge but before the patient needs full-time care. This is a challenging time for the patient, medical staff, and family because it usually requires significant transitions in treatment and daily care. Since most families can't afford to care for their loved one full-time, a professional caregiver is often hired.
While professional caregivers are trained in navigating the particularities of dementia, they also introduce a few unavoidable obstacles. First, they become the mediator between all other stakeholders: the patient, their family, their doctors, etc. They must be able to translate medical information in understandable terms to all of these parties. This presents a second problem: the ability of a dementia patient to absorb and apply guidance changes rapidly. One day the patient may be able to retain verbal reminders while the next day they may need written cues as well. This problem area is where my team and I decided to focus because it presented a lot of opportunities for design intervention.
A new way of life
Dementia is a chronic condition whose symptoms can vary drastically throughout its progression. This inconsistency makes it difficult to give medical care to patients and impractical to design any sort of hard and fast interventions. This burden often falls on a typically overlooked stakeholder: the caregiver, whether in the family or professional.
Needing to narrow down somewhere in the disease's timeline, My team and I decided to target the two intermediate stages of dementia caregiving (shifting responsibility and increasing demand) for multiple reasons. These stages mark the time between when symptoms are becoming a daily challenge but before the patient needs full-time care. This is a challenging time for the patient, medical staff, and family because it usually requires significant transitions in treatment and daily care. Since most families can't afford to care for their loved one full-time, a professional caregiver is often hired.
While professional caregivers are trained in navigating the particularities of dementia, they also introduce a few unavoidable obstacles. First, they become the mediator between all other stakeholders: the patient, their family, their doctors, etc. They must be able to translate medical information in understandable terms to all of these parties. This presents a second problem: the ability of a dementia patient to absorb and apply guidance changes rapidly. One day the patient may be able to retain verbal reminders while the next day they may need written cues as well. This problem area is where my team and I decided to focus because it presented a lot of opportunities for design intervention.

“Most times with dementia long-term memory is intact until the very end. So getting people to tell stories from their own past to think in the moment is helpful in grounding them in reality before you have a conversation that requires rational thought. There is potential to see the progress of the patient, not just deterioration.”
Excerpt from a interview with a professional caregiver
Excerpt from a interview with a professional caregiver
“Patient trust serves to reinforce the functioning of a health partnership, thereby increasing the probability of patient satisfaction, treatment adherence, and improved health status, while decreasing the likelihood of withdrawing from a health plan.”
(Pearson & Raeke, 2000)
(Pearson & Raeke, 2000)
“Storytelling had specific benefits for residents (increased creativity, improved quality of life, positively altered behavior, and involvement in meaningful activity), and caregivers (learning new practices, developing a deeper understanding of residents, involvement in meaningful activity, and thinking creatively around programmatic challenges).”
(George & Houser, 2014)
(George & Houser, 2014)

RESEARCH
An unexpected requirement for a patient's treatment adherence is trust. Similar to bedside manner, a patient's trust in their caretaker affects their medical data retention and understanding. Unfortunately, there is little trust between patients and professional caregivers, often complete strangers. We determined that building trust, empathy, and rapport between the patient and their caregiver would be the best way to improve information delivery and retention.
Through interviews with professional and primary caregivers and secondary research, we found that storytelling is a proven method of building trust. We were essentially connecting two thoroughly researched topics. First, storytelling is helpful for dementia patients as a social activity because it boosted their creativity and helped build empathy with their caregiver. And second, increased trust and understanding between a patient and their caregiver improves data delivery, retention, and adherence because the data can be contextualized and personalized (Fiske et al., 2019).
Reaching an understanding
An unexpected requirement for a patient's treatment adherence is trust. Similar to bedside manner, a patient's trust in their caretaker affects their medical data retention and understanding. Unfortunately, there is little trust between patients and professional caregivers, often complete strangers. We determined that building trust, empathy, and rapport between the patient and their caregiver would be the best way to improve information delivery and retention.
Through interviews with professional and primary caregivers and secondary research, we found that storytelling is a proven method of building trust. We were essentially connecting two thoroughly researched topics. First, storytelling is helpful for dementia patients as a social activity because it boosted their creativity and helped build empathy with their caregiver. And second, increased trust and understanding between a patient and their caregiver improves data delivery, retention, and adherence because the data can be contextualized and personalized (Fiske et al., 2019).

Giving it dimension
When considering what format would be best to introduce storytelling into a caregiver's visit with a dementia patient, my team and I kept returning to one point mentioned in our early interviews: “The only thing better than visual aids would be 3D models to help explain something. It engages spatial thinking that many people with certain kinds of dementia have an impairment.” We thought that a three-dimensional object would be both innovative and intuitive for people without much experience with a smartphone. Our final form, the cube, could easily be flipped and turned, paralleling the unfolding nature of stories without superfluous interaction with a digital user interface. Our user testing of the object came to the same conclusion: “This is a whole different area you are working in is their spatial cognitive response and long term memory with the photos. You are also doing short term memory by having pictures on different surfaces and having patients remember where they are.”








FINAL PRODUCT
On a typical day with a dementia patient, a caregiver will begin their visit by engaging them in a story. A prompt will appear on the cube's home screen to initiate the conversation. These prompts can be customized— preferences like complexity and dependence on memory change automatically with disease progression or manually adjusted.
While the patient tells their story to the caregiver, the cube will begin recording and act as a visual mediator. Pieces of the story appear as images on the faces of the cube once they're mentioned to spark further conversation. Once the patient is finished with their story, the caregiver can archive it or provide feedback on the efficacy of the prompt.
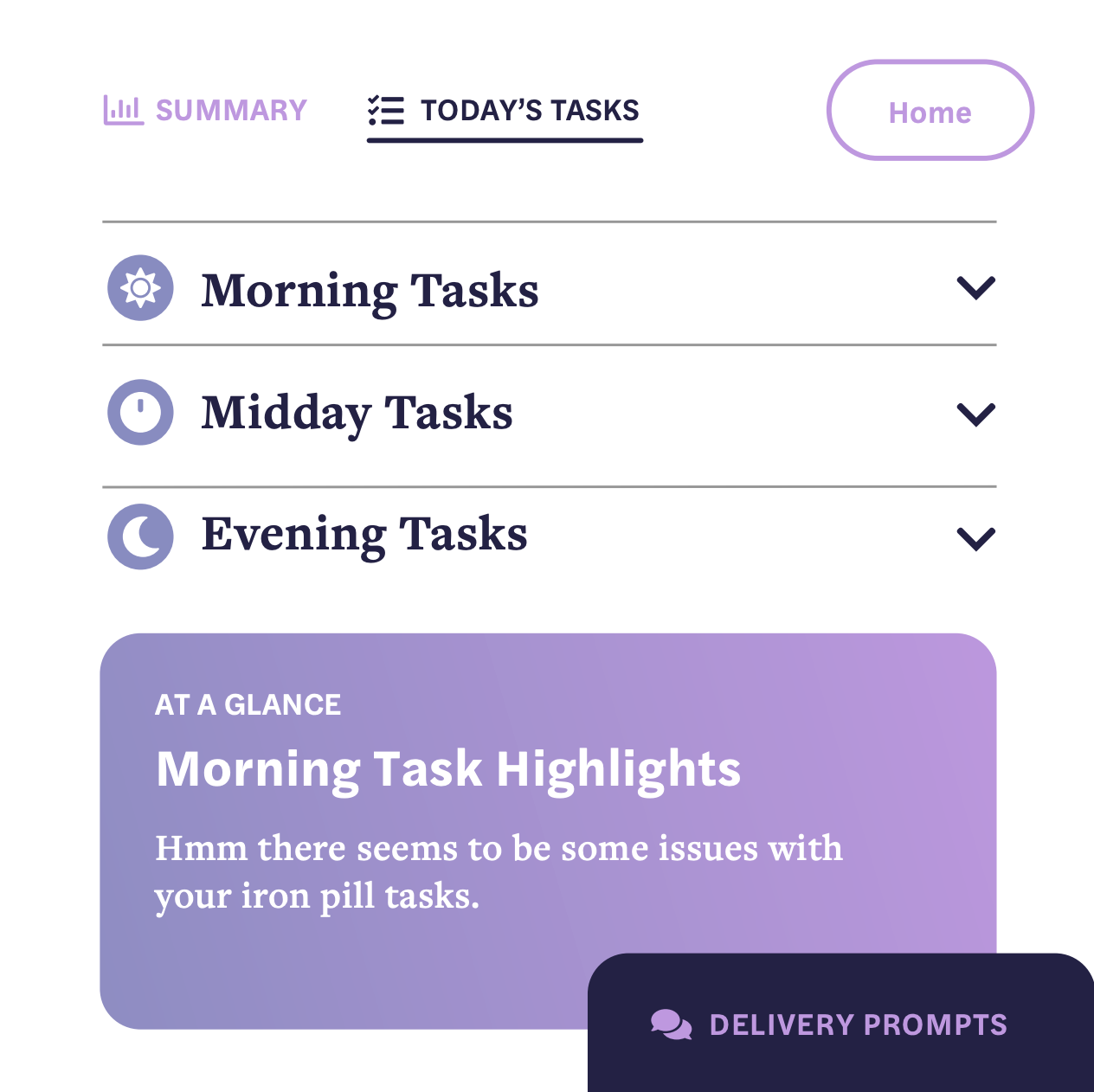
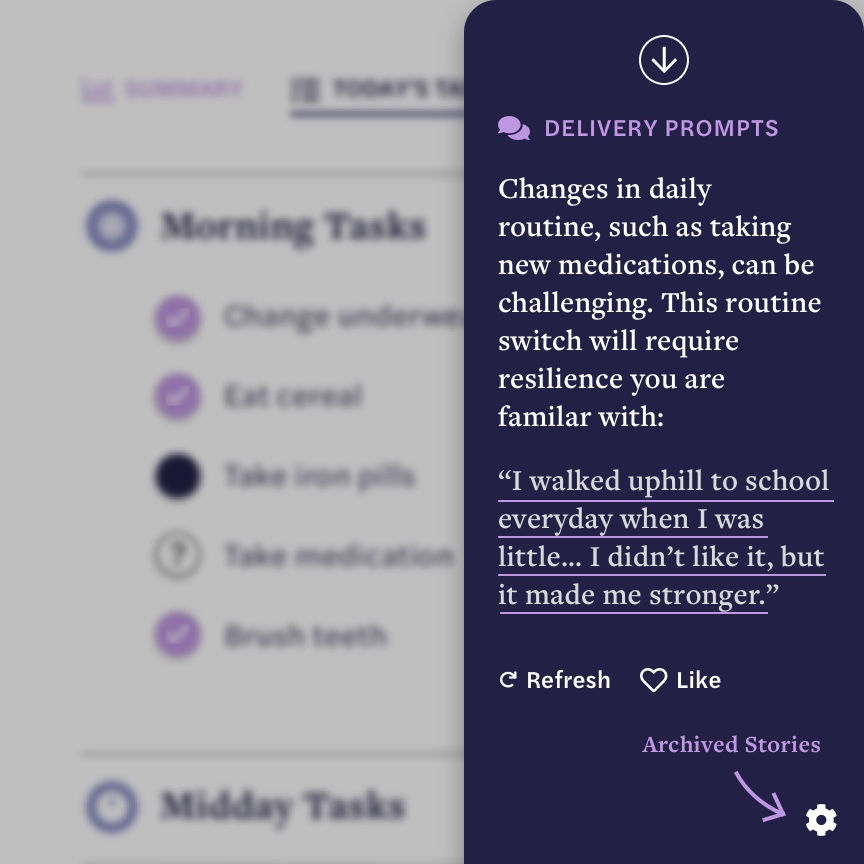
After the storytelling is over, the caregiver reviews with the patient their daily tasks and medical data. The involves relaying recommendations from their doctor, ensuring the patient is taking their medications, checking to see if their house is in order, etc. If the caregiver runs into any issues, the cube recommends a delivery strategy based on the disease progression and past storytelling sessions. For example, if the patient is having trouble adjusting to a new medication routine, the cube may suggest the caregiver remind them of a childhood story they previously told with a moral of resilence. Using past recorded stories to resolve current challenges builds rapport between the caregiver and their patient while also boosting retention and adherence.
Spinning a yarn
On a typical day with a dementia patient, a caregiver will begin their visit by engaging them in a story. A prompt will appear on the cube's home screen to initiate the conversation. These prompts can be customized— preferences like complexity and dependence on memory change automatically with disease progression or manually adjusted.
While the patient tells their story to the caregiver, the cube will begin recording and act as a visual mediator. Pieces of the story appear as images on the faces of the cube once they're mentioned to spark further conversation. Once the patient is finished with their story, the caregiver can archive it or provide feedback on the efficacy of the prompt.
After the storytelling is over, the caregiver reviews with the patient their daily tasks and medical data. The involves relaying recommendations from their doctor, ensuring the patient is taking their medications, checking to see if their house is in order, etc. If the caregiver runs into any issues, the cube recommends a delivery strategy based on the disease progression and past storytelling sessions. For example, if the patient is having trouble adjusting to a new medication routine, the cube may suggest the caregiver remind them of a childhood story they previously told with a moral of resilence. Using past recorded stories to resolve current challenges builds rapport between the caregiver and their patient while also boosting retention and adherence.
Wider implcations
This design intervention introduces new narrative and spatial methods in dementia care. Leveraging human connection to build empathy through storytelling, especially in three-dimensional form, has never been researched before. It also increases awareness of caregiver’s needs, an often overlooked stakeholder in the medical field. Moving forward, we wonder: How could this three-dimensional, spatial system be used in other contexts? How could our device adapt throughout the entire disease and beyond? How can machine learning further navigate the nuances of dementia?
WORKS CITED
Fels, D. I., & Astell, A. J. (2011). Storytelling as a Model of Conversation for People With Dementia and Caregivers. American Journal of Alzheimer’s Disease & Other Dementias, 535–541.
Fiske, A., Prainsack, B., & Buyx, A. (2019). Data Work: Meaning-Making in the Era of Data-Rich Medicine. Journal of Medical Internet Research, 21(7).
George, D. R., & Houser, W. S. (2014). “I’m a Storyteller!”: Exploring the Benefits of TimeSlips Creative Expression Program at a Nursing Home. American Journal of Alzheimer’s Disease & Other Dementias, 678–684.
Pearson, S. D., & Raeke, L. H. (2000). Patients’ trust in physicians: Many theories, few measures, and little data. Journal of General Internal Medicine, 15(7), 509–513.